Early versus Late initiation of direct oral Anticoagulants in post-ischaemic stroke patients with atrial fibrillatioN (ELAN): an international, multicentre, randomised-controlled, two-arm, assessor-blinded trial
Please find more information on www.clinicaltrials.gov
Aim of the study
The ELAN trial aims to estimate the net benefit of early versus late (current standard practice) initiation of direct oral anticoagulants (DOACs) in patients with acute ischaemic stroke related to atrial fibrillation.
Background
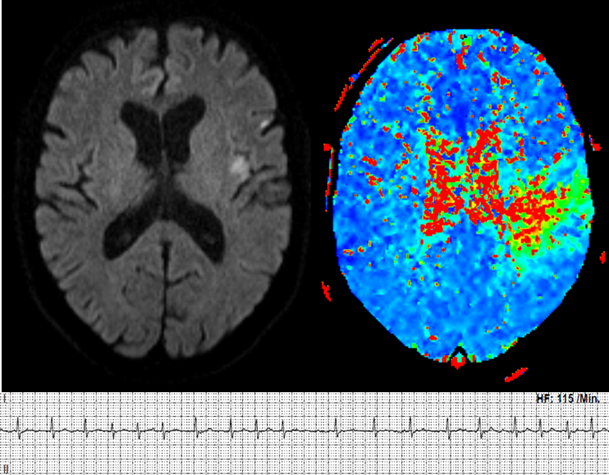
Figure 1: Acute embolic stroke due to M3-occlusion with diffusion-perfusion mismatch on MRI due to newly detected atrial fibrillation on ECG in a 63-year-old-patient.
When to start anticoagulation in patients with an acute ischaemic stroke and atrial fibrillation is a relevant unanswered question in clinical practice. Figure 1 shows an acute embolic stroke due to atrial fibrillation on MRI. It was shown that DOACs are highly effective for secondary stroke prevention in these patients, but DOACs were never initiated <7 days after stroke onset in recent trials.
-
Outcome
The primary outcome is a composite of major bleeding, recurrent ischaemic stroke, systemic embolism and/or vascular death at 30 ± 3 days after randomisation.
Secondary outcomes are: mRS and compliance at 30 ± 3 days after randomisation as well as mRS, NIHSS, major bleeding, recurrent ischaemic stroke, systemic embolism, all-cause mortality, bleeding, myocardial infarction, vascular death, major cardiovascular events, silent brain lesion and favourable outcome (mRS) at 90 ± 7 days after randomisation.
Trial design
The trial is an international, multicentre, randomised-controlled, two-arm, assessor-blinded trial lasting four years.
Please check the key inclusion and exclusion criteria below.

- Age ≥18 years
- Acute ischemic stroke
- Atrial fibrillation (permanent, persistent, or paroxysmal spontaneous)
- Agreement of treating physician to prescribe direct oral anticoagulants (DOACs)

- Atrial fibrillation due to reversible causes
- Valvular disease, Mechanical heart valves, Mitral stenosis, Aortic dissection
- Atrial fibrillation (AF) and conditions other than AF that require therapeutic anticoagulation or heparin, Dual antiplatelet therapy
- Serious bleeding, Parenchymal haemorrhage, Severe comorbid condition, Renal insufficiency, Tumour, Cerebral vasculitis, Endocarditis
- Pregnant or lactating women
- Contradiction to direct oral anticoagulants (DOACs)
We will start the recruitment in October 2017 with currently approximately 80 sites in Switzerland and European countries (https://www.elan-trial.ch/participating-sites/).
Treatment/Control Groups
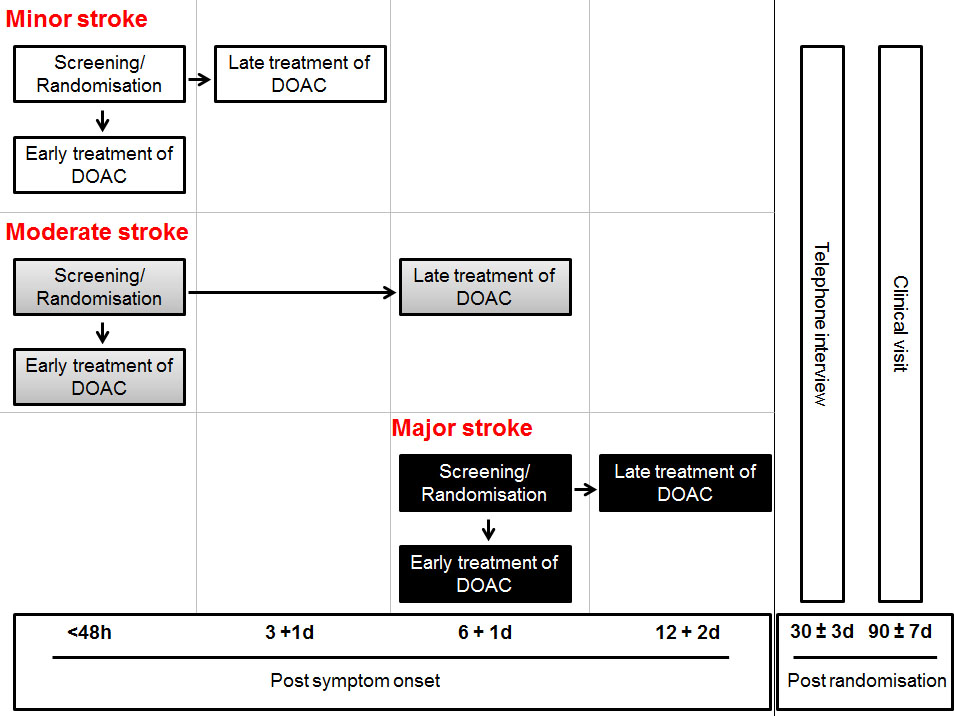
Figure 2: Trial schedule; DOAC, direct oral anticoagulants; Tel., telephone; h, hours; d, days.
In total 2000 patients, with the experimental arm (early treatment; 1000) and control arm (late treatment, 1000). Patients in the early treatment and the late treatment (control arm) will receive DOACs for prevention of stroke and systemic embolism in patients with atrial fibrillation. The initiation of DOACs will vary depending on lesion size as shown in Figure 2.
Patients with early treatment will receive DOACs within 48 hours after symptom onset (minor and moderate ischaemic stroke) or at day 6 + 1 day after symptom onset (major ischaemic stroke).
Patients with late treatment (which represents the current standard practice in the clinics) will receive DOACs as follows: minor ischaemic stroke after day 3 + 1 day, moderate ischaemic stroke after day 6 + 1 day and major ischaemic stroke after day 12 + 2 day).
All DOACs with marketing authorization in Switzerland and the EU for prevention of stroke and systemic embolism in patients with atrial fibrillation can potentially be used in this trial, i.e the following and potential generics with the dose (as indicated in the product sheets):
- Rivaroxaban (Xarelto®), 20 mg 1x / day
- Dabigatran (Pradaxa®), 150 mg 2x / day
- Apixaban (Eliquis®), 5 mg 2x / day
- Edoxaban (Lixiana®), 60 mg 1x / day
ELAN stroke size classification
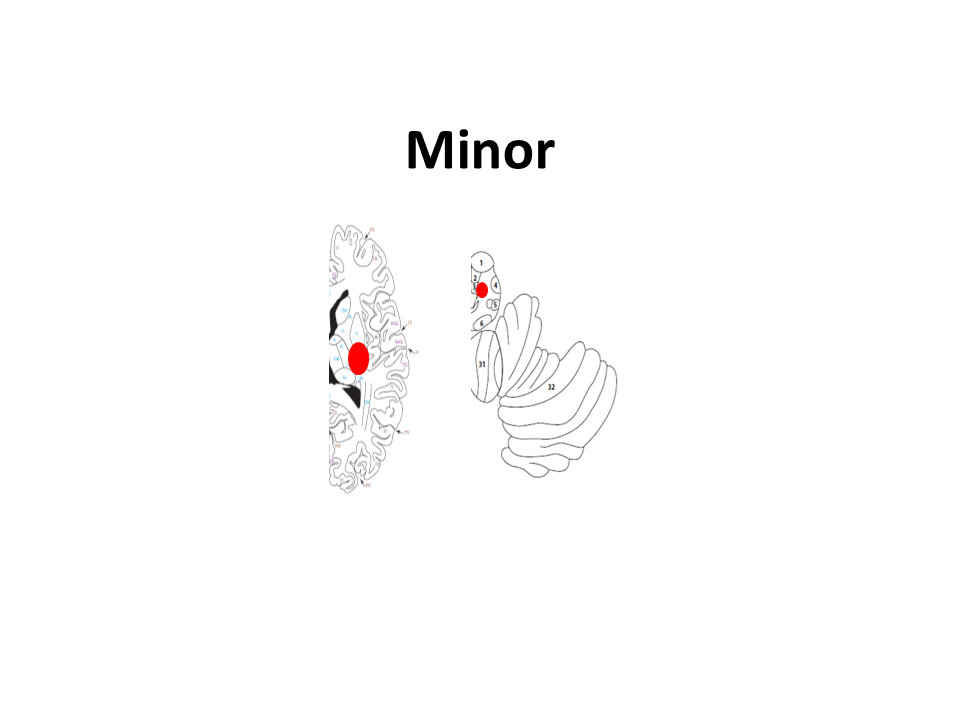
Minor
lesion is ≤1.5 cm in anterior or posterior circulation
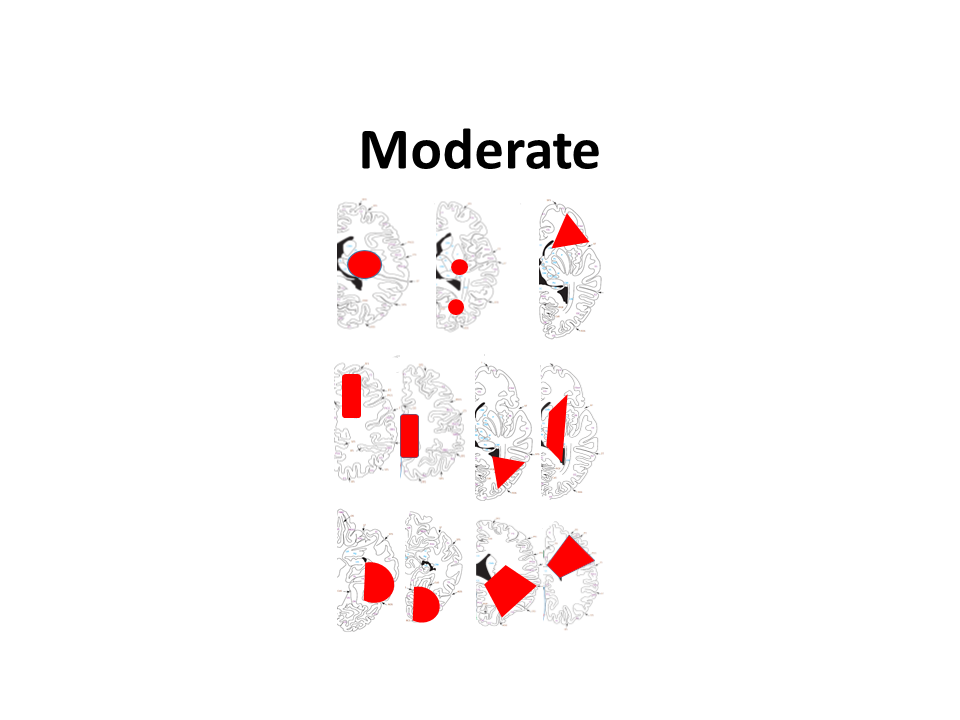
Moderate
lesion is in a cortical superficial branch of the middle cerebral artery (MCA), in the MCA deep branch, in the internal border zone territories, in a cortical superficial branch of posterior cerebral artery, in a cortical superficial branch of the anterior cerebral artery
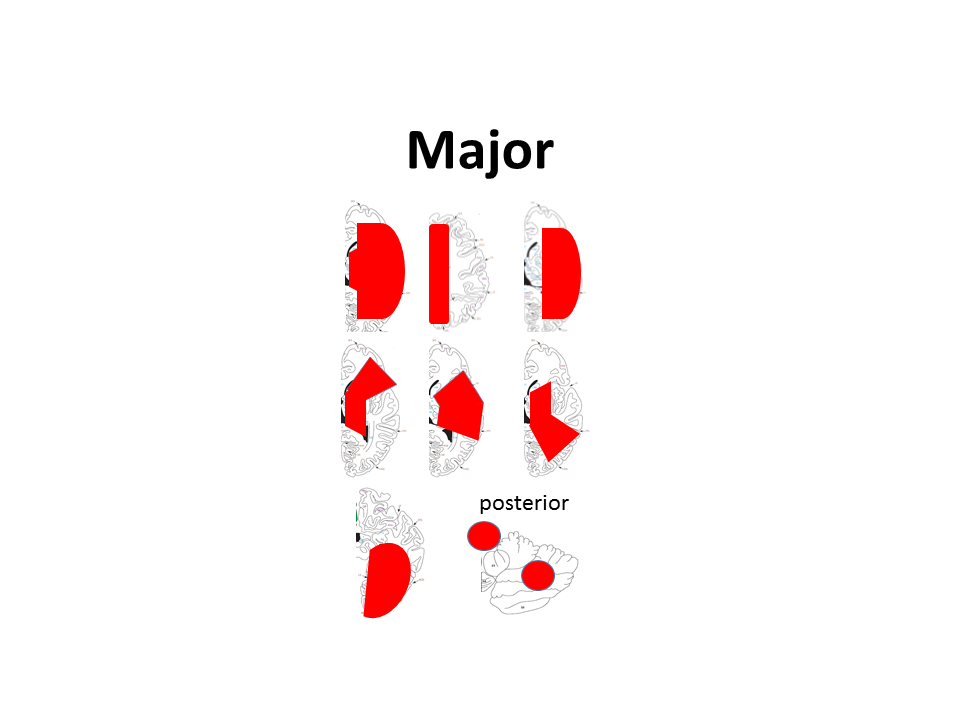
Major
anterior: lesion involves the complete territory of MCA, posterior cerebral artery, or anterior cerebral artery, in two cortical superficial branches of MCA, in a cortical superficial branch of MCA associated to the MCA deep branch, or in >1 artery territory (e.g. MCA associated to anterior cerebral artery territories posterior: lesion is ≥1.5 cm in the brainstem or Cerebellum
cave: multiple minor tiny spots (embolic shower) = minor stroke
cave: two minor lesions = moderate stroke (the sum of the lesions)
cave: two moderate lesions = major stroke
{kind=link}
Steering committee

Prof. Dr. med. Urs Fischer
University Hospital Bern

Prof. Dr. med. Jesse Dawson
University Hospital Glasgow

Prof. Dr. med. Daniel Strbian
University Hospital Helsinki

Dr. med. Maurizio Paciaroni
University Hospital Perugia

Prof. Dr. med. Götz Thomalla
University Clinics Hamburg-Eppendorf

Prof. Dr. med. Georg Ntaios, PhD
University of Thessaly

Prof. Dr. med. Leo Bonati
University Hospital Basel

Prof. Dr. med. Patrik Michel
University Hospital Lausanne

Prof. Dr. med. Krassen Nedeltchev
Cantonal Hospital Aarau

PD Dr. med. Sven Trelle
CTU Bern, University Bern

PD Dr. med. Thomas Gattringer
University Clinics Graz

Dr. Else Charlotte Sandset
Oslo University Hospital – Ullevål
Funding
The ELAN Trial is funded by the Swiss National Science Foundation and the Swiss Heart Foundation.
Top recruiting sites in Switzerland, the United Kingdom and Finland have applied for matching funds to continue with the research work.
Impact
This pragmatic investigator-initiated international trial will add evidence to the best time of starting DOAC after ischaemic stroke in patients with atrial fibrillation. If earlier initiation of DOACs in patients with ischaemic stroke related to atrial fibrillation is shown to be safe and efficacious, this could have a major impact on better treatment adherence, length of hospital stay and patient outcome.
Endorsement
The ELAN Trial is endorsed by the Stroke Alliance For Europe
![]()